Primary Assessment – J-A-C-C-O-L-D
J-A-C-C-O-L-D is a quick visual and clinical screening tool during primary assessment in children: Jaundice, Anaemia, Cyanosis, Clubbing, Oedema, Lymphadenopathy, Dehydration.
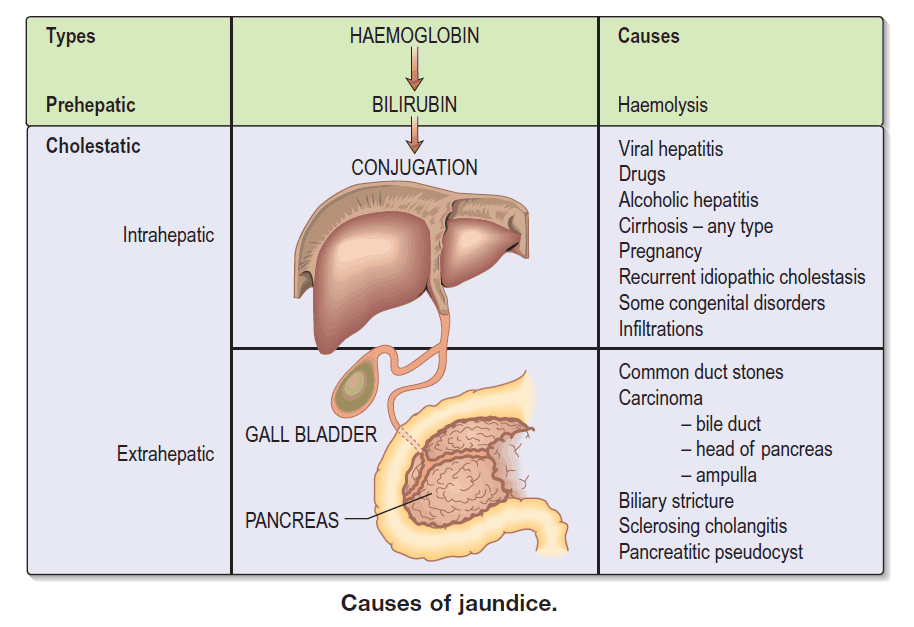
J – Jaundice in Paediatric Patients
Clinical features:
- Yellow discoloration of sclerae and skin.
- Dark urine, pale or putty-coloured stools.
Associated symptoms:
- Fatigue, poor feeding or failure to thrive.
- Abdominal pain or hepatomegaly.
- Pruritus (especially in cholestatic disease).
Common causes (by age):
- Neonates: physiological jaundice, sepsis, haemolysis, biliary atresia.
- Infants/children: viral hepatitis, autoimmune or metabolic liver disease, haemolytic anaemias, biliary obstruction.
Key ED investigations:
- Liver function tests, conjugated vs unconjugated bilirubin.
- FBC, reticulocyte count, Coombs test if haemolysis suspected.
- Abdominal ultrasound if obstructive or structural disease suspected.
A – Anaemia in Paediatric Patients
Clinical features:
- Pallor (conjunctivae, palms, mucosa), tachycardia.
- Fatigue, irritability, poor feeding or exercise intolerance.
Common causes:
- Nutritional deficiencies – iron, folate, B12.
- Haemolysis – hereditary, autoimmune, infections.
- Chronic disease, renal disease, malignancy, blood loss.
Key ED investigations:
- Full blood count and blood film.
- Reticulocyte count, iron studies; consider haemolysis screen if indicated.
- Stool occult blood or other tests guided by history.
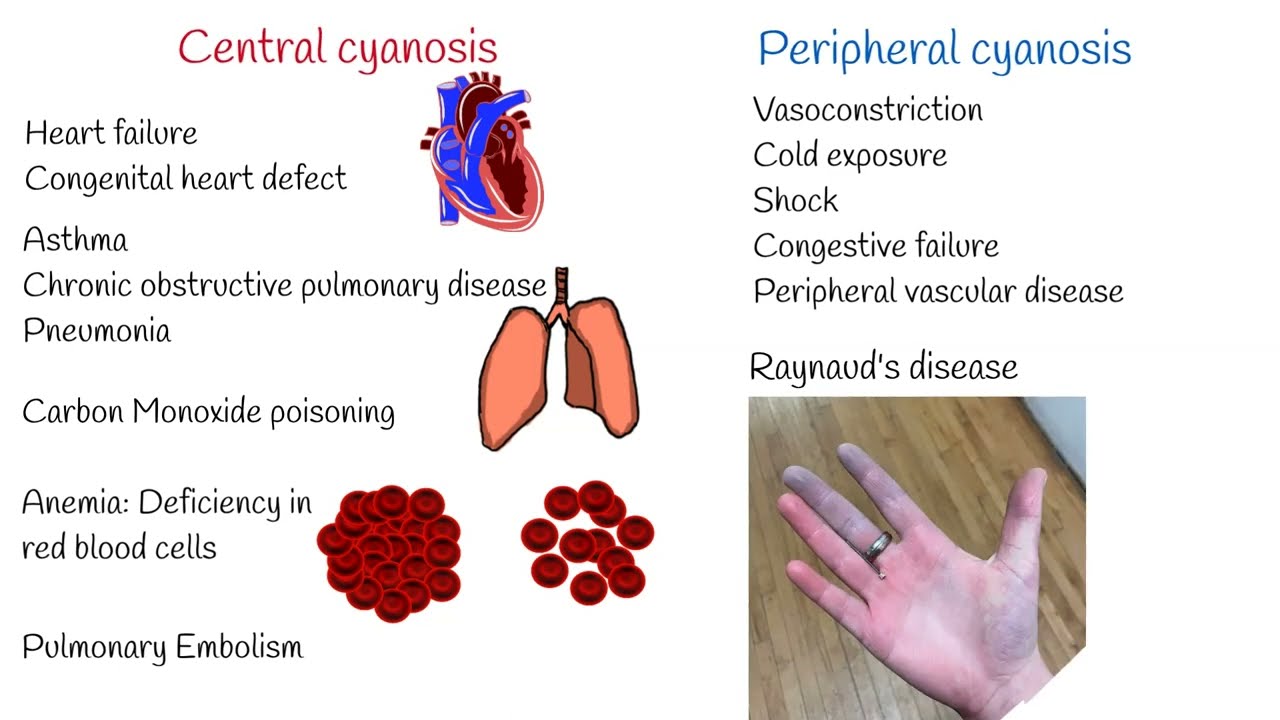
C – Cyanosis in Paediatric Patients
Clinical features:
- Bluish discoloration of lips, tongue, nail beds, or extremities.
- May be central (tongue) or peripheral (extremities).
Associated symptoms:
- Tachypnoea, respiratory distress.
- Irritability, poor feeding, lethargy.
- Failure to thrive, recurrent chest infections.
Important causes:
- Congenital heart disease (cyanotic lesions).
- Severe pneumonia, bronchiolitis, asthma, foreign body.
- Sepsis, shock, or methemoglobinaemia (rare).
Key ED investigations:
- Pulse oximetry and blood gas (consider co-oximetry if available).
- Chest X-ray, ECG; consider echocardiogram (often via cardiology).
- Basic bloods and lactate if septic or shocked.
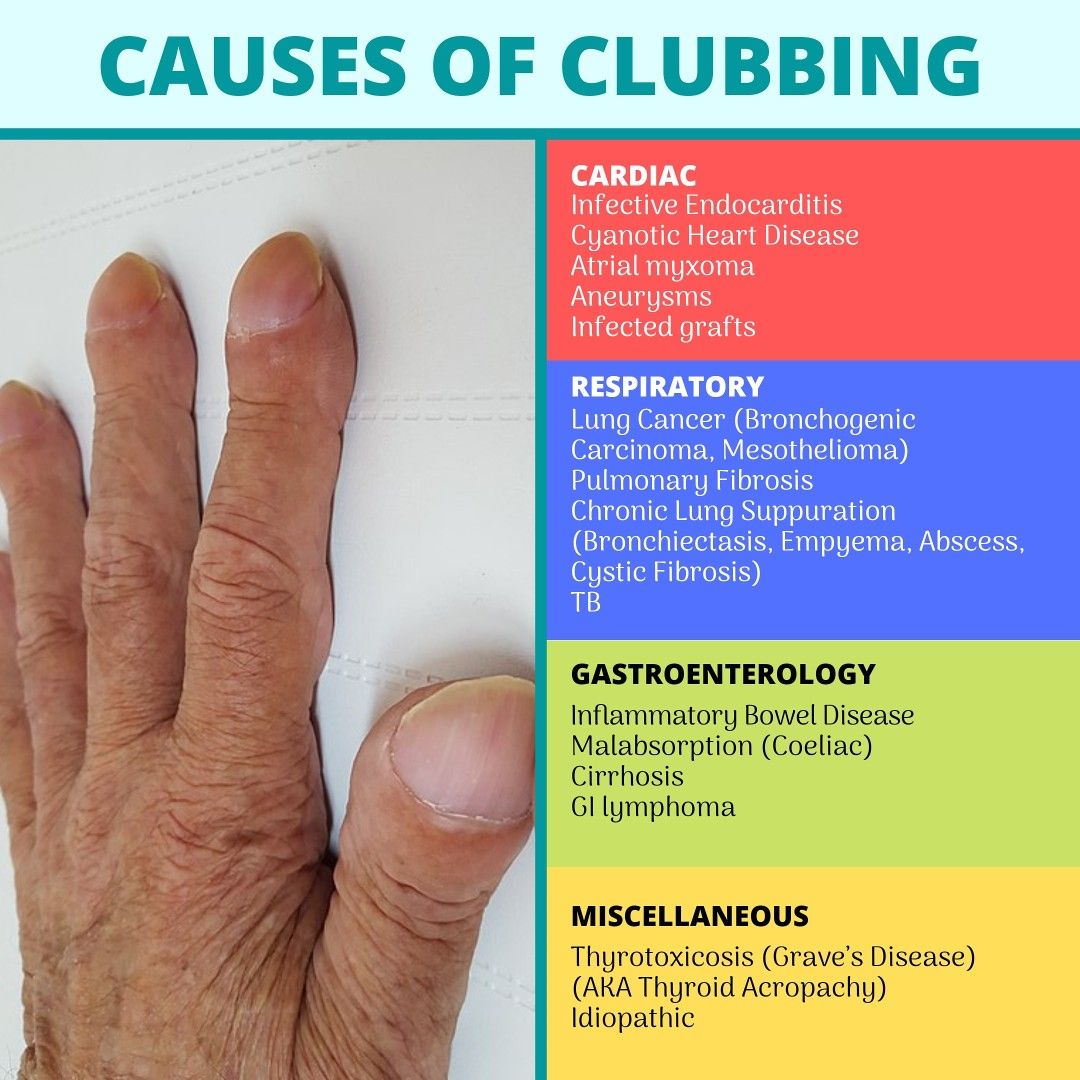
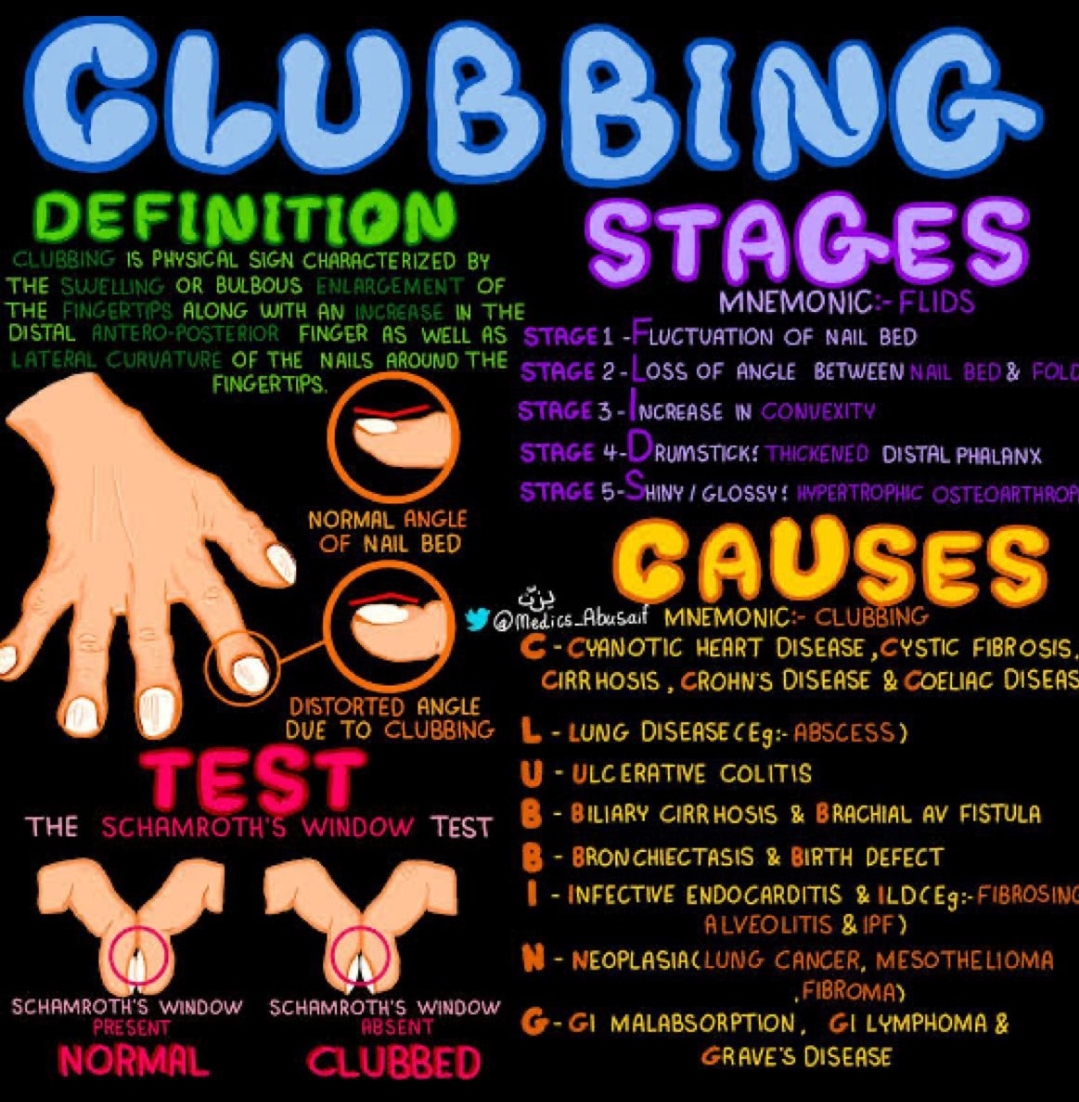
C – Digital Clubbing in Paediatric Patients
Clinical features:
- Bulbous enlargement of distal phalanges, “drumstick” fingers.
- Loss of nail–fold angle, spongy nail beds.
Suggestive of chronic disease:
- Chronic suppurative lung disease (e.g., cystic fibrosis, bronchiectasis, TB).
- Cyanotic congenital heart disease.
- Chronic liver disease, inflammatory bowel disease, some malignancies.
Key ED considerations: clubbing is usually chronic – it should prompt you to look for long-standing cardiopulmonary or systemic illness and confirm appropriate follow-up.
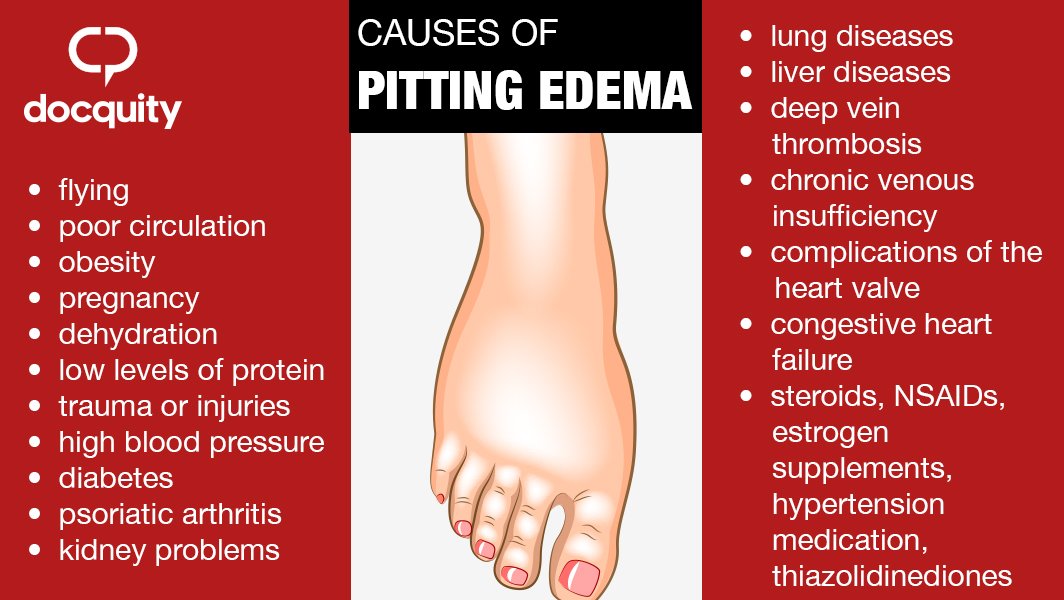
O – Oedema in Paediatric Patients
Clinical features:
- Swelling of feet, ankles, legs, periorbital area or abdomen (ascites).
- Pitting oedema over bony prominences.
Common causes:
- Renal disease (e.g., nephrotic syndrome, nephritis).
- Cardiac failure, congenital heart disease.
- Liver disease, severe malnutrition, protein-losing enteropathy.
Key ED investigations:
- Urinalysis (protein, blood), U&E, creatinine.
- Liver function tests, albumin.
- Chest X-ray, echocardiogram where indicated.
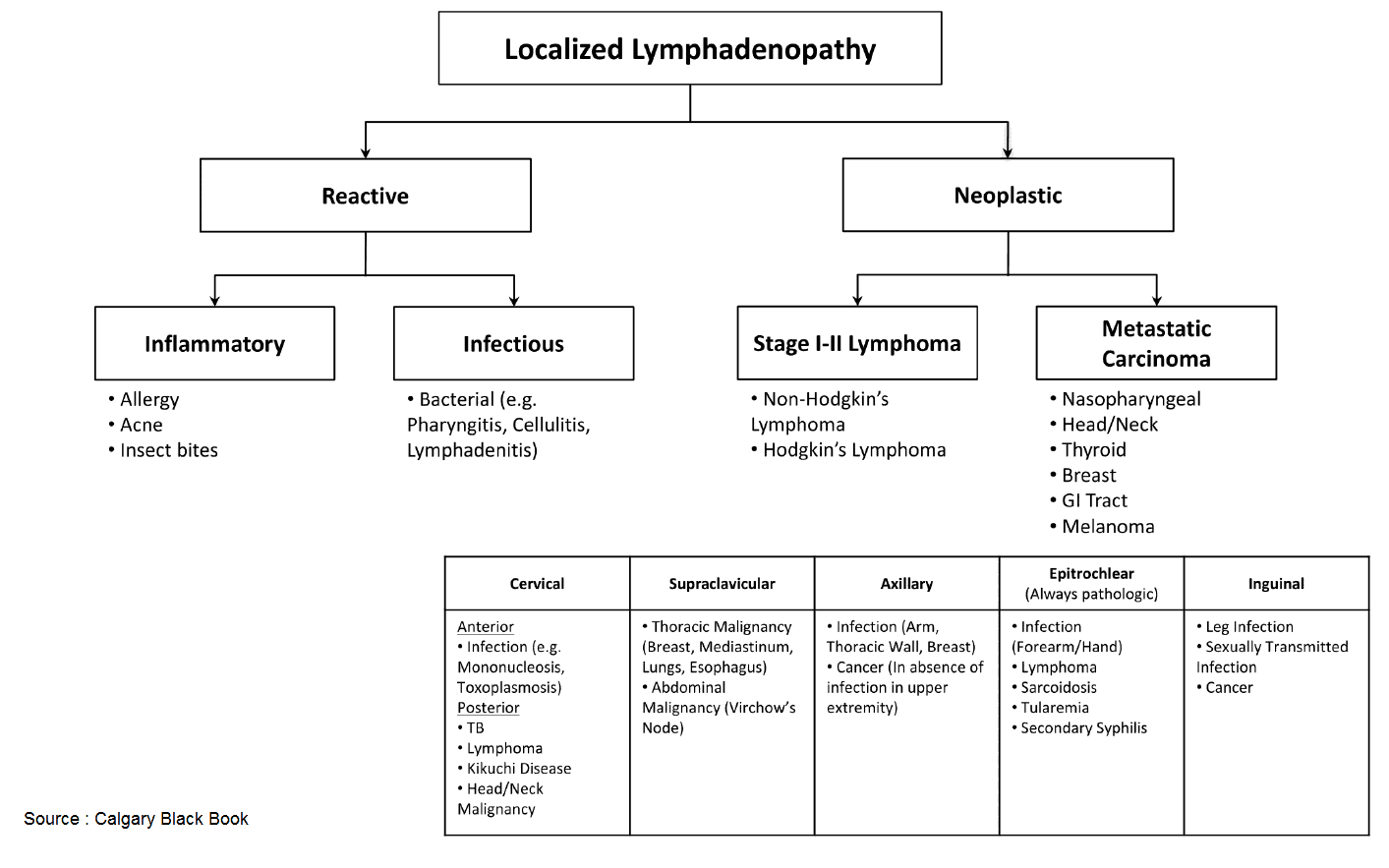
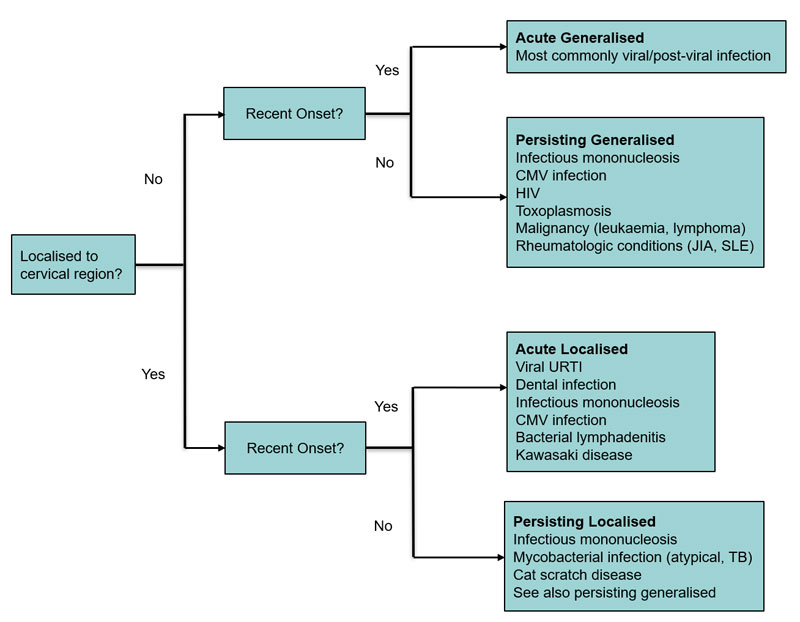
L – Lymphadenopathy in Paediatric Patients
Clinical features:
- Enlarged lymph nodes (commonly cervical, axillary, inguinal).
- Nodes may be tender, mobile, or fixed depending on cause.
Common causes:
- Self-limiting viral or bacterial infections.
- Suppurative nodes, TB, atypical mycobacterial infection.
- Haematological malignancies or systemic inflammatory disease (less common but important).
Key ED considerations:
- Look for red flags – weight loss, night sweats, persistent fever, very large or hard, fixed nodes.
- Document size, site, tenderness, and overlying skin changes.
Suggested investigations: (guided by history)
- FBC, inflammatory markers, TB screening where appropriate.
- Ultrasound of node(s) if concern for abscess or malignancy.
D – Dehydration in Paediatric Patients
Key clinical signs:
- Dry mucous membranes, dry lips and tongue.
- Reduced tears, decreased urine output or dark urine.
- Sunken eyes, sunken fontanelle in infants.
- Tachycardia, cool peripheries, prolonged capillary refill in more severe cases.
Symptoms (depending on age and severity):
- Thirst, irritability, lethargy.
- Dizziness, weakness, headache in older children.
- Reduced activity, poor feeding.
Common causes:
- Gastroenteritis (vomiting and diarrhoea).
- Fever with poor intake, excessive sweating.
- Diabetes (e.g., new-onset diabetes or DKA), diuretics or other medications.
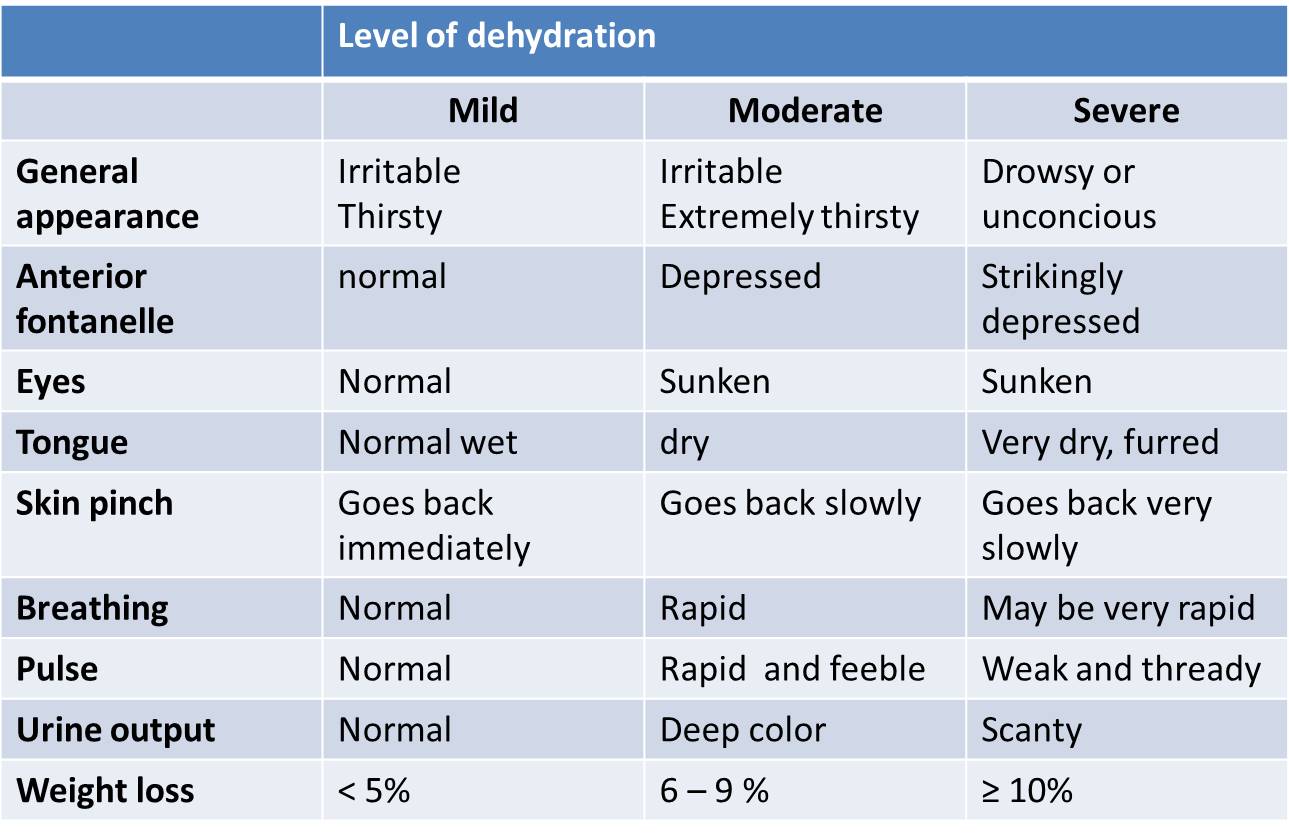
Clinical Grading (Bedside)
- Mild: Slightly dry mucosa, normal vitals, alert, urine output slightly reduced.
- Moderate: Dry mucosa, reduced skin turgor, sunken eyes/fontanelle, tachycardia, irritable.
- Severe: Very dry mucosa, markedly reduced turgor, deeply sunken eyes/fontanelle, weak rapid pulse, cold peripheries, lethargy or altered mental status.
Emergency Department Management
- Mild dehydration: Oral rehydration solution (ORS); small frequent amounts; continue feeding when possible.
- Moderate dehydration: ORS if tolerated; consider IV fluids if ongoing losses or inability to drink; monitor vitals and urine output closely.
- Severe dehydration / shock: Treat as an emergency – IV or IO access, isotonic fluid bolus (e.g. 10–20 mL/kg) over 10–20 minutes, then reassess and repeat as per local protocol.
Relevant investigations (based on severity and cause):
- U&E, creatinine, glucose, bicarbonate.
- Blood gas (venous/arterial) to assess acidosis and lactate.
- Urinalysis (ketones, specific gravity), stool studies if indicated.
Intravenous Rehydration – ED Approach
Choice of fluid:
- Isotonic crystalloids (e.g. 0.9% saline, Ringer’s lactate) are first-line in most children with significant dehydration or shock.
- Avoid hypotonic fluids for initial resuscitation.
- Use specialised protocols for DKA, hypernatraemia, or complex electrolyte disturbances.
Typical ED strategy:
- Start with a bolus of 10–20 mL/kg isotonic crystalloid over 10–20 minutes in shock; reassess after each bolus.
- Once circulation stabilised, calculate maintenance plus replacement according to local guidelines and ongoing losses.
- Monitor heart rate, blood pressure, capillary refill, mental status, urine output and weight (if possible).